2011 - 10th Meeting - IHCTAS
This page contains exclusive content for the member of the following sections: TTS, IHCTAS. Log in to view.
Posters
2.27 - POSTERIOR RECTUS SHEATH AS A VASCULARIZED COMPOSITE ALLOGRAFT IN MULTIVISCERAL BOWEL TRANSPLANTATION
Presenter: Kadiyala, Ravindra, Durham, NC, USA
Authors: Kadiyala Ravindra, Scott Hollenbeck, Deepak Vikraman, Abigail Martin, Todd Brennan, Bradley Collins, Detlev Erdmann, Debra Sudan
POSTERIOR RECTUS SHEATH AS A VASCULARIZED COMPOSITE ALLOGRAFT IN MULTIVISCERAL BOWEL TRANSPLANTATION
Kadiyala Ravindra1, Scott Hollenbeck1, Deepak Vikraman1, Abigail Martin1, Todd Brennan1, Bradley Collins1, Detlev Erdmann1, Debra Sudan1.
1Department of Surgery, Duke University, Durham, NC, USA.
Introdution: Congenital anomalies such Prune belly syndrome are associated with poor abdominal wall musculature. This poses problems when these patients receive small bowel or multivisceral transplantation. A recent innovation uses the vascularized anterior rectus sheath in continuity with the liver (Fig.1). We applied this in a child with Prune Belly syndrome.
Patient and Method: A 2 year male with Prune belly syndrome listed to receive a multivisceral graft (Liver with small bowel). His abdominal wall was extremely lax – particularly on the right side. We conducted a fresh cadaver dye study to document the presence of blood flow to the posterior rectus sheath from the hepatic artery through branches in the falciform ligament.
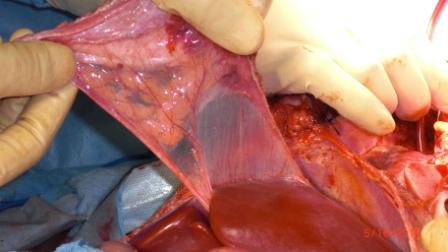
At organ procurement the posterior rectus sheath was harvested in continuity with the falciform ligament attached to the multivisceral graft. After implantation of the graft, the rectus sheath appeared well vascularized and was used to restore the abdominal wall (Fig.2).
Results: The abdominal wall healed uneventfully. At 8 months, the child is on enteral nutrition with restoration of abdominal wall.
Conclusions: Posterior rectus sheath above the umbilicus receives blood flow from the hepatic artery, enabling its use as a composite tissue graft with a liver or mutivisceral allograft. This procedure has a potential application in patients undergoing multivisceral transplantation when the abdominal wall structure and function has been compromised by developmental defects or scarring from previous surgeries.

Important Disclaimer
By viewing the material on this site you understand and accept that:
- The opinions and statements expressed on this site reflect the views of the author or authors and do not necessarily reflect those of The Transplantation Society and/or its Sections.
- The hosting of material on The Transplantation Society site does not signify endorsement of this material by The Transplantation Society and/or its Sections.
- The material is solely for educational purposes for qualified health care professionals.
- The Transplantation Society and/or its Sections are not liable for any decision made or action taken based on the information contained in the material on this site.
- The information cannot be used as a substitute for professional care.
- The information does not represent a standard of care.
- No physician-patient relationship is being established.
Contact
Address
The Transplantation Society
International Headquarters
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada