
Transplantation Direct August 2021 Issue
JUST RELEASED - TRANSPLANTATION DIRECT - AUGUST ISSUE
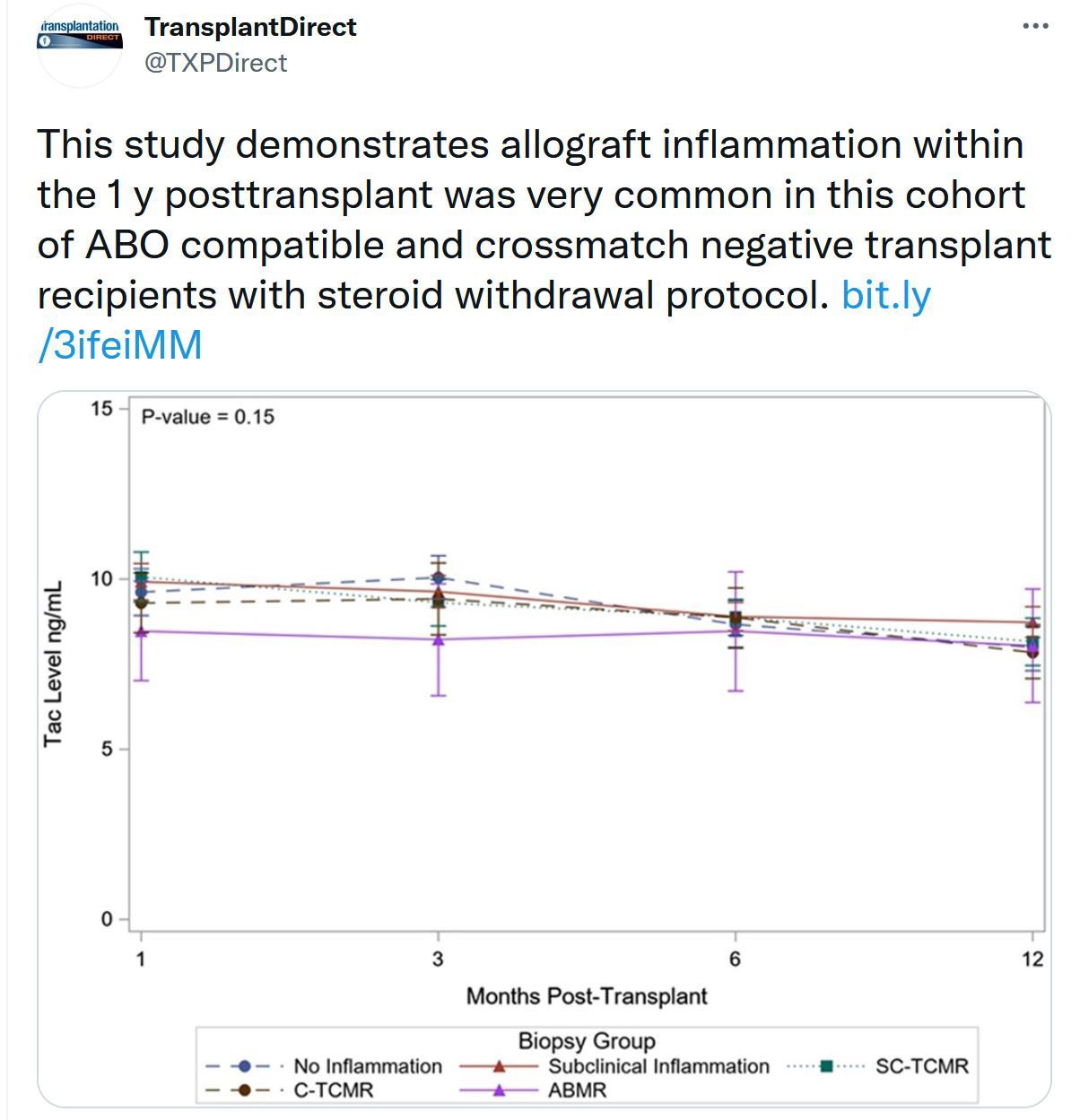
The August issue of Transplantation Direct is online. This is an issue touching many areas of the transplantation field, including kidney, liver, lung, heart, intestinal, bone marrow and stem cell transplantation, as well as xenotransplantation. We offer reviews on monoclonal gammopathy of undetermined significance in kidney transplantation (Tx) and on protocols for anonymous living liver donation. There are articles on the topic on normothermic perfusion of DCD kidneys -- one relates to GWAS of key mitochondrial pathways in pig studies, and the other on regional organ perfusion programs. Another article looks at the effect of nephron mass in DCD kidneys regarding pediatric donation to adults. The subjects of other kidney Tx studies include HLA incompatible transplantation in sensitized patients, the impact of Mayo Adhesive Probability score in living donor transplantation, transplanting patients with pre-Tx pulmonary hypertension, outcomes in patients receiving dual basiliximab and ATG induction, and the association of HLA alleles with post-Tx diabetes. Liver transplant articles touch on allograft dysfunction related to DCD vs DBD grafts, long-term results from a prolonged-release tacrolimus trial, desensitizing recipients with preformed DSA, surgical aspects of interposition grafts for split livers, and transplanting organs from a SARS-CoV-2 positive living donors. Other topics relate to biomarkers for restrictive allograft syndrome after lung Tx, veno-arterial ECMO to bridge heart Tx, GvHD after intestinal Tx, and long-term effects of ABO mismatching on stem cell Tx. For those interested in xenotransplantation, mechanisms of neutrophil-induced tissue damage are explored. To unpack all the details, please visit our open access Transplantation Direct website.
TTS Masterclasses: Outcome Reporting Series Begins August 18
TTS Members can now register for FREE for the last two Masterclass Series on Transplant Immunology and Outcome Reporting. Members must pre-register to attend the live Masterclasses.

TTS is pleased to announce that the remaining two Masterclass Series (Transplant Immunology Series & Outcome Reporting Series) have been granted European CME credits (ECMEC®s) by the European Accreditation Council for Continuing Medical Education (EACCME®).
Attendance at the live Masterclasses is mandatory to receive the certificate.
Upcoming Masterclasses



Upcoming August 18 TID-TTS Webinar
August 18, 2021
09:00 (-4 GMT - Montreal time)







Contact
Address
The Transplantation Society
International Headquarters
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada
Используйте Вавада казино для игры с бонусом — активируйте промокод и начните выигрывать уже сегодня!